Skip to content
Search for:
Borrow
Browse Catalog
Get a Card
Patron Guidelines
Patron Item Request
Libby
Hoopla
Beanstack
Indiana Digital Library
Library of Things
Visit
Hours & Location
Library Holiday Closings
Services & Resources
Services Available
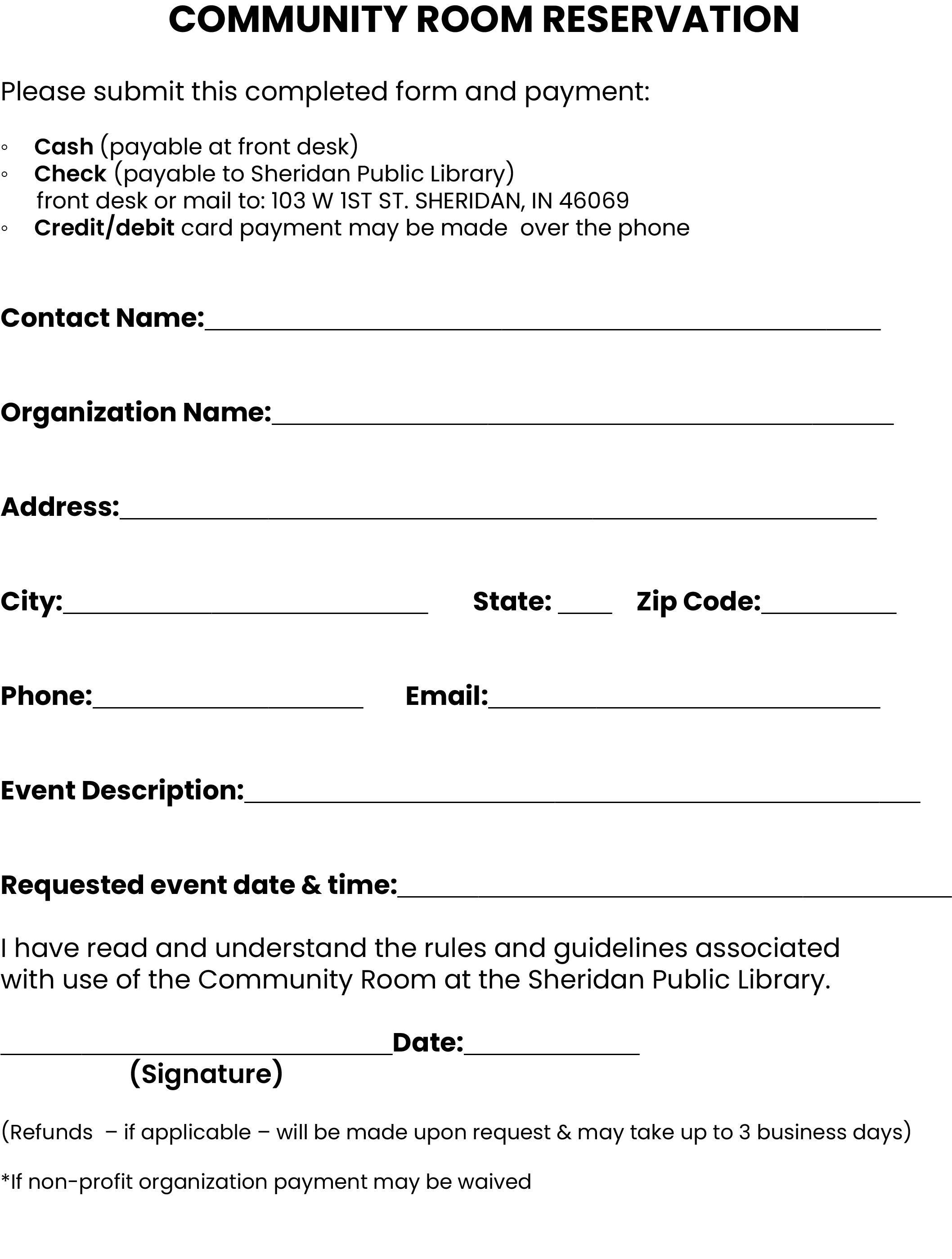
Reserve Community Room
Resources & Links
Kids & Teens
Preschool Programs
Reading Programs
Kids & Teen Events
Kids & Teen Resources
STEAM Grab & Go Kits
Story Time to Go Kits
Toniebox & Tonies
Adults
About
Library Staff
Policies & Information
Volunteer at SPL
Monthly Newsletter Signup
Current Newsletter
Wowbrary
RESERVATION
Lindsay Spencer
2024-10-09T15:15:16-04:00
[bws_pdfprint]
Page load link
Go to Top
 [bws_pdfprint]
[bws_pdfprint]